Middle-aged diabetic patient presenting with shortness of breath. Clinical evidence of pulmonary oedema.
Describe and interpret this ECG
ECG ANSWER and INTERPRETATION
Main Abnormal Findings
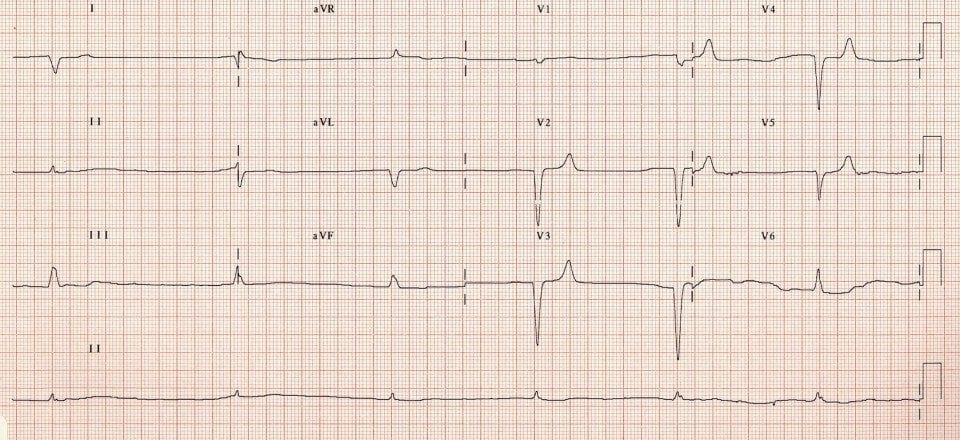
- Severe bradycardia of 36 bpm
- Rhythm is difficult to ascertain — appears irregular (?slow AF) although there are some small-voltage P waves seen in V1-2
- Broad QRS complexes with an atypical LBBB morphology
- Subtle symmetrical peaking (“tenting”) of the T waves in V2-5
Diagnosis
The combination of bradycardia, flattening and loss of P waves, QRS broadening and T wave abnormalities is highly suspicious for severe hyperkalaemia. This patient had a potassium of 8.0 in the context of anuric renal failure.
CLINICAL PEARLS
When you see the combination of…
- Bradycardia
- Blocks — e.g. AV block, bundle branch blocks
- Bizarre QRS complexes
…. think hyperkalaemia!
The push-pull effect
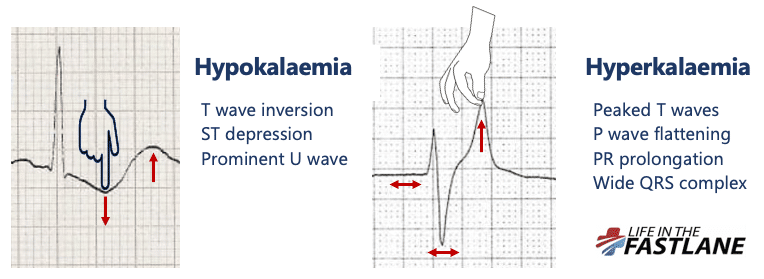
- Hypokalaemia creates the illusion that the T wave is “pushed down”, with resultant T-wave flattening/inversion, ST depression, and prominent U waves
- In hyperkalaemia, the T wave is “pulled upwards”, creating tall “tented” T waves, and stretching the remainder of the ECG to cause P wave flattening, PR prolongation, and QRS widening
Emergency Physician in Prehospital and Retrieval Medicine in Sydney, Australia. He has a passion for ECG interpretation and medical education | ECG Library |
MBBS DDU (Emergency) CCPU. Adult/Paediatric Emergency Medicine Advanced Trainee in Melbourne, Australia. Special interests in diagnostic and procedural ultrasound, medical education, and ECG interpretation. Co-creator of the LITFL ECG Library. Twitter: @rob_buttner