85-year old patient presenting with nausea, vomiting and visual disturbance. Looks clinically dehydrated. Describe the ECG.
Describe and interpret this ECG
ECG ANSWER and INTERPRETATION
Main Abnormalities
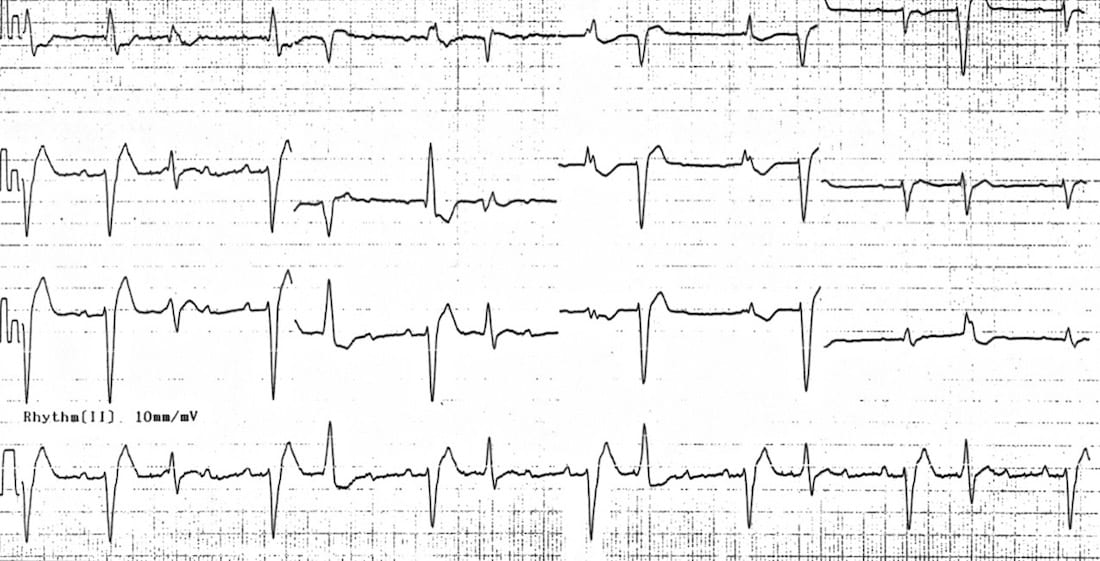
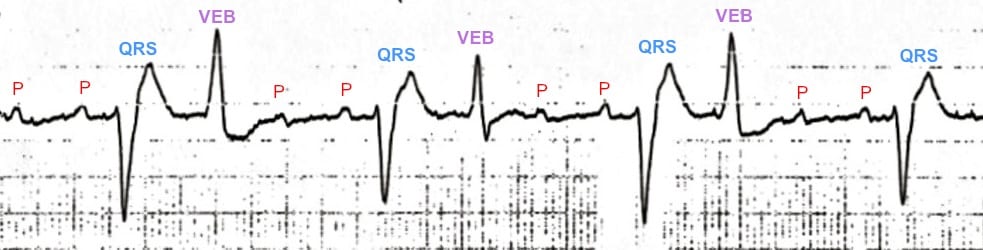
- Atrial tachycardia, with regular P waves visible at ~ 160 bpm (many of the P waves are hidden within T waves and VEBs)
- Evidence of high-grade AV block — there is a 4:1 conduction ratio between P waves and QRS complexes, with a QRS rate of ~ 40 bpm
- Frequent ventricular ectopic beats occurring in a pattern of ventricular bigeminy
- Alternating LBBB and RBBB morphology, with the conducted QRS complexes demonstrating RBBB morphology (RSR’ in V1) and the VEBs demonstrating LBBB morphology (dominant S wave in V1)
Diagnosis
The combination of…
- Atrial tachycardia
- Frequent ventricular ectopic beats
- High-grade AV block
… is almost pathognomonic of severe digoxin toxicity.
CLINICAL PEARLS
ECG Features of Digoxin Toxicity
Digoxin toxicity produces a wide variety of dysrhythmias, due to:
- Increased automaticity of atrial and ventricular tissues — via actions at the Na/K and Na/Ca exchangers causing increased intracellular calcium and therefore increased spontaneous depolarisation of cardiac pacemaker cells
- Decreased AV conduction — via increased vagal tone at the AV node
Digoxin toxicity therefore usually produces some combination of:
Characteristic ECG patterns include:
NB. Digoxin toxicity should not be confused with digoxin effect (= “sagging” ST depression and T-wave inversion in patients on therapeutic doses of digoxin; not predictive of toxicity).
Emergency Physician in Prehospital and Retrieval Medicine in Sydney, Australia. He has a passion for ECG interpretation and medical education | ECG Library |
MBBS DDU (Emergency) CCPU. Adult/Paediatric Emergency Medicine Advanced Trainee in Melbourne, Australia. Special interests in diagnostic and procedural ultrasound, medical education, and ECG interpretation. Co-creator of the LITFL ECG Library. Twitter: @rob_buttner