Previously well 70 year old man presents to peripheral hospital with central chest pain and diaphoresis

Describe and interpret this ECG
ECG ANSWER and INTERPRETATION
Rate:
Rhythm:
Axis:
Intervals:
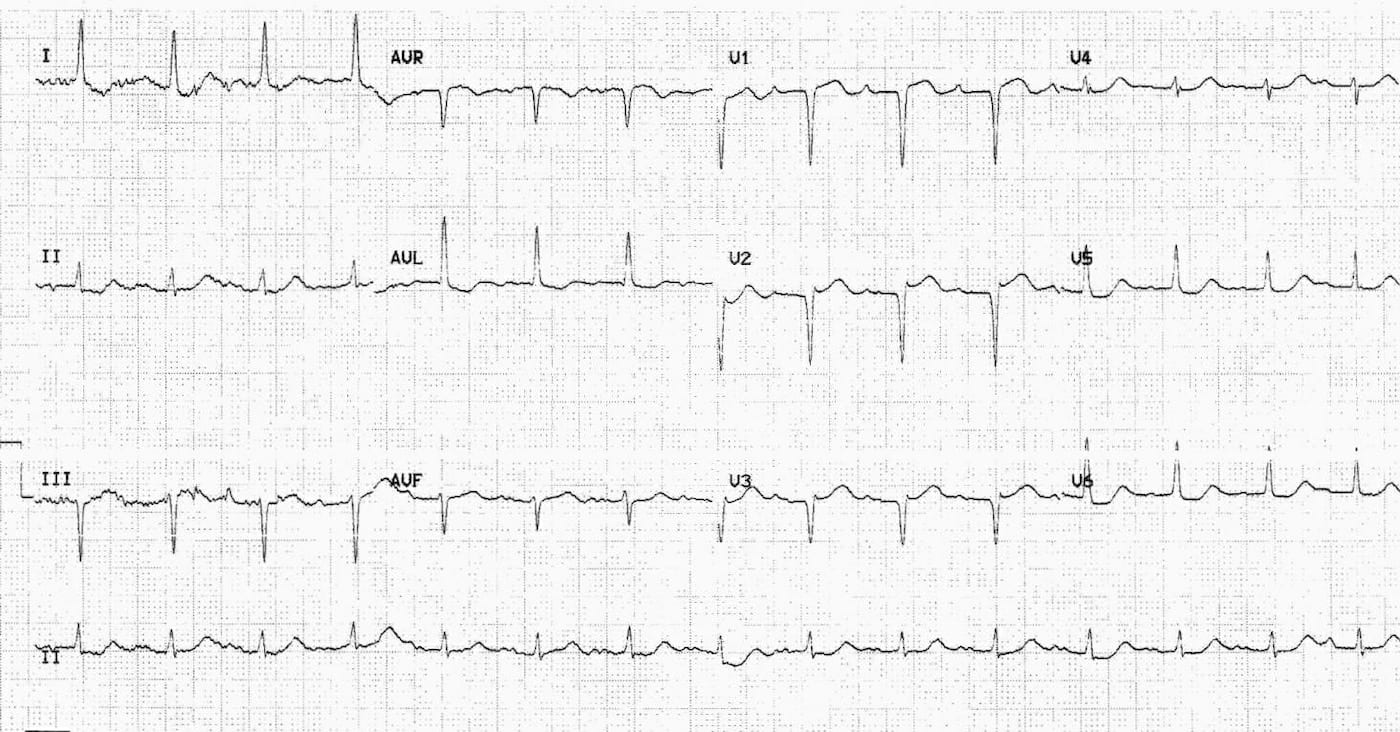
- PR – Prolonged (200 – 240ms)
- QRS – Normal (80ms)
- QT – 440ms (QTc Bazett 310ms)
Segments:
- ST Elevation aVR (3-4 mm) V1 (3mm) V2 (2mm)
- ST Depression I, II, aVF, aVL, V4-6
Additional:
- Notched p wave in lead II, possible biphasic P wave in V1
- Poor r wave progression
Interpretation:
- Most marked abnormality is ST elevation in aVR, V1-2, with ST Depression I, II, aVF, aVL, V4-6
- Also 1st Degree AV block and possible left atrial enlargement (p mitrale)
- This pattern is most consistent with a LMCA occlusion (STE aVR >/= V1)
- LMCA occlusion associated with a high mortality (aVR STE>1.5mm up to 70% mortality)
- Could also be proximal LAD lesion or severe 3-vessel disease
Management
- Urgent liaison with cardiology is required
- Need to discuss reperfusion therapy based on available resources / local policies
- Consideration of likelihood of requiring CABG is needed as this may affect initial drug therapy, particularly clopidogrel or prasugrel due to increased incidence of post operative bleeding
ECG 2
ECG INTERPRETATION
Key features:
- ST Elevation V1-2 (1mm)
- ST Depression I, aVL, V5-6
Interpretation:
- ST Elevation & Depression Resolving when compared with ECG 1
What happened next ?
- Patient was reviewed and admitted by cardiology team
- Planned for urgent angiography
- Pt declined intervention
- Re-presented with APO and cardiogenic shock
FURTHER READING
Life in the Fast Lane
Dr Smith’s ECG Blog
Articles
- Yamaji H, Iwasaki K, Kusachi S, Murakami T, Hirami R, Hamamoto H, Hina K, Kita T, Sakakibara N, Tsuji T. Prediction of acute left main coronary artery obstruction by 12-lead electrocardiography. ST segment elevation in lead aVR with less ST segment elevation in lead V(1). J Am Coll Cardiol. 2001 Nov 1;38(5):1348-54
- Kosuge M, Ebina T, Hibi K, Morita S, Endo M, Maejima N, et al. An early and simple predictor of severe left main and/or three-vessel disease in patients with non-ST-segment elevation acute coronary syndrome. Am J Cardiol. 2011 Feb 15;107(4):495-500
Emergency Medicine Specialist MBChB FRCEM FACEM. Medical Education, Cardiology and Web Based Resources | @jjlarkin78 | LinkedIn |