These ECGs are from a 58 yr old male reviewed in a rural setting, approximately ~2500 km from the nearest tertiary centre. He complained of intermittent atypical chest pain over a period of several weeks without any cardiac risk factors.
At the clinic serial ECGs were performed
- What do you think of the ECGs ?
- What advice would you give assuming you were the clinician at the tertiary receiving hospital who was contacted regarding this case ?

Describe and interpret these ECGs
ECG ANSWER and INTERPRETATION
ECG 1
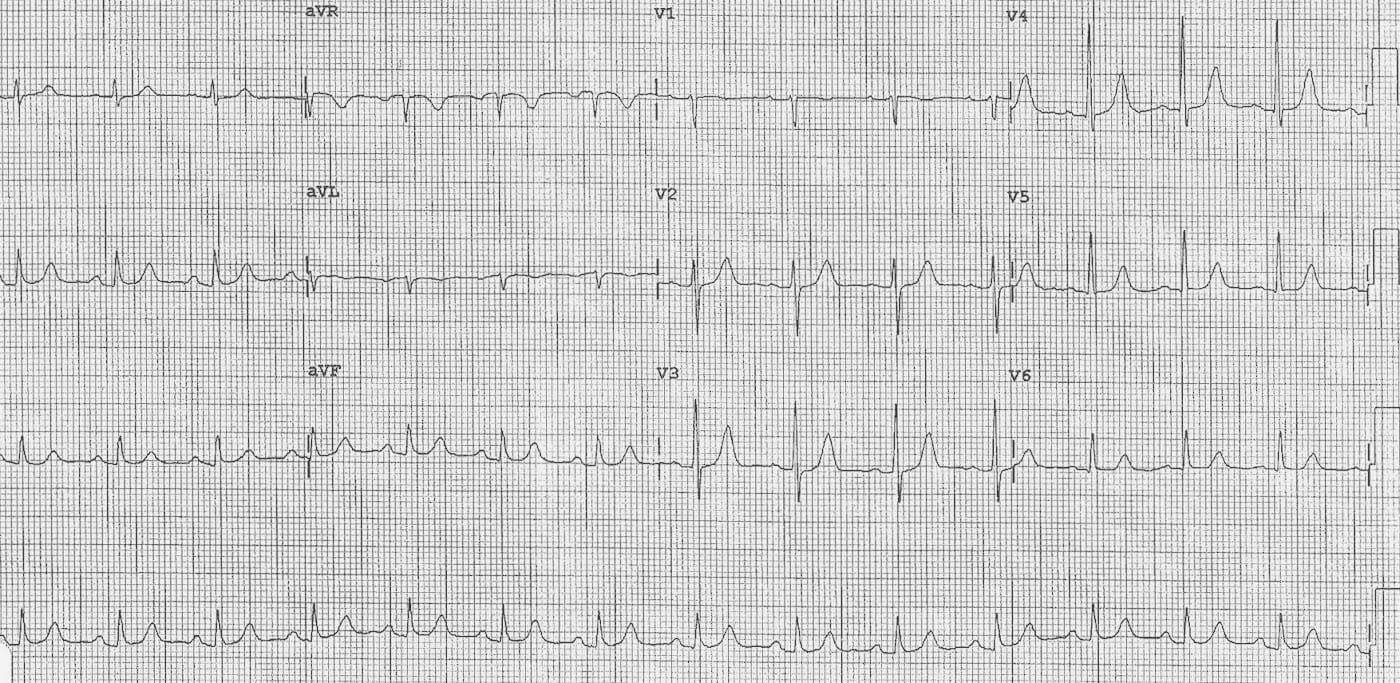
Rate:
Rhythm:
Axis:
Intervals:
- PR – Normal (~160-200ms)
- QRS – Normal (80ms)
- QT – 340ms (QTc Bazett ~ 390 ms)
Segments:
- Slight Saddling ST segments leads II, III, aVF
ECG 2
Rate:
Rhythm:
Axis:
Intervals:
- PR – Normal (~180 ms)
- QRS – Normal (80ms)
- QT – 360ms (QTc Bazett ~ 360 ms)
Segments:
- Slight Saddling ST segments leads I, aVL
Additional:
- T Wave Inversion Leads III, aVF
Initial interpretation:
- This ECG was interpreted as having dynamic ST change ? ACS.
- The patient was anticoagulated and transferred by air, ~2500 km, to a tertiary centre for further management.
CLINICAL PEARLS
…but let’s look again:
- The answer is somewhat less pathological.
- There is an axis change between the 2 ECGs which is a little odd
- Look at the complexes in leads III and you can see not only has the T wave become inverted but so has the P wave and QRS complex
- Compare leads aVL & aVF between the two ECGs and we can see these leads have been swapped
The ECG changes are due to a LA / LL lead reversal
- Leads aVL & aVF swap places
- Leads I & II swap places
- Lead III becomes completely inverted
- Lead aVR remains unchanged
- No change in the precordial leads
Emergency Medicine Specialist MBChB FRCEM FACEM. Medical Education, Cardiology and Web Based Resources | @jjlarkin78 | LinkedIn |