59yr old male who presented to the Emergency Department following 2 episodes of syncope. He had a long history of infrequent unexplained syncope over the prior 15 years.
His only past medical history is diet controlled T2DM and he was taking no regular medications.
ECG on presentation
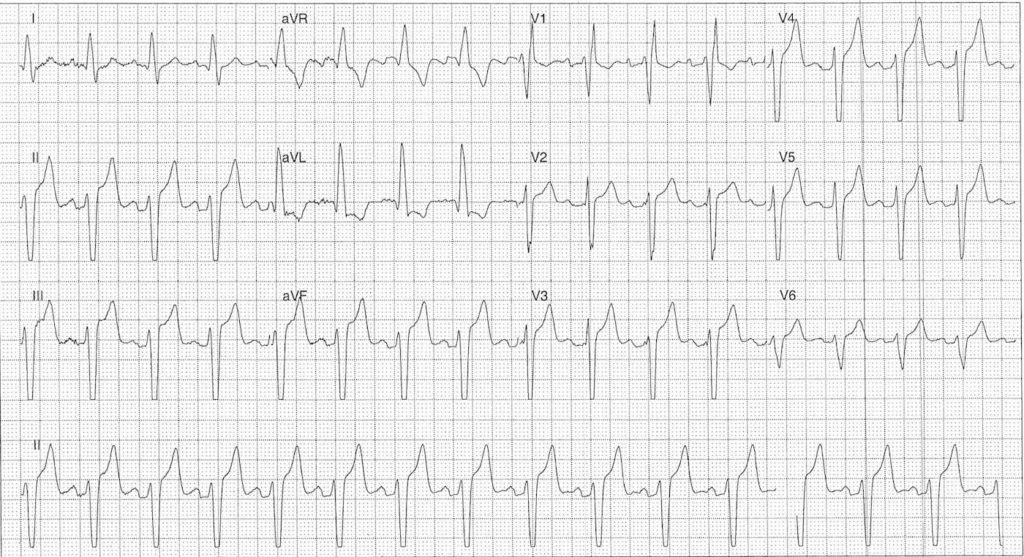
** NOTE this is a non-diagnostic ECG recording as it was generated retrospectively from the rhythm telemetry unit
Describe and interpret this ECG
ECG ANSWER and INTERPRETATION
Key features:
- Sinus rhythm rate ~90 bpm
- Left axis deviation
- RBBB Morphology
- Prominent T waves and ST elevation in leads II, III, aVF, V2-5 with high voltage complexes
- This ECG was generated using the monitor (non-diagnostic) algorithm. The filter applied in this mode is 0.5 to 40 Hz which can over- or under-estimate low frequency portions of the ECG including the ST segment.
- The diagnostic algorithm filter performs at 0.05 to 150 Hz.
- For a somewhat complicated overview of ECG filtering check out:
- Borderline 1st degree AV block
Interpretation:
- Bifascicular Block
- Borderline PR prolongation
- Requires cardiology referral for monitoring and consideration of PPM insertion given history of syncope
- ST / T wave changes without chest pain or electrolyte abnormality – related to ECG filtering algorithm
ECG with palpitations
The patient complained of palpitations. Due to rate and rhythm change a rhythm strip was automatically generated
ECG ANSWER and INTERPRETATION
Key features:
- Atrial rate 136 bpm
- Ventricular rate 27 bpm
- AV Dissociation
- Broad Complex QRS
Impression:
- Complete heart block
- Ventricular escape rhythm
Interpretation:
- Compared with rhythm strip above
- Complete heart block
- AV Dissociate with ventricular escape rhythm, rate 24 bpm
- Slowing of atrial rate now ~115 bpm
CLINICAL OUTCOME
What happened next?
The patient was treated with atropine followed by isoprenaline infusion.
The next day he underwent an uneventful dual chamber PPM insertion. A subsequent echo showed was normal with an ejection fraction of 64%.
On review of his medical records prior ECG’s had shown alternating left and right bundle branch blocks confirming progressive conducting system disease.
Further reading:
Emergency Medicine Specialist MBChB FRCEM FACEM. Medical Education, Cardiology and Web Based Resources | @jjlarkin78 | LinkedIn |