Suspect and look for right ventricular (RV) infarction in all patients with inferior STEMI.
ECG diagnostic criteria
In patients with inferior STEMI, RV infarction is suggested by:
- ST elevation in V1
- ST elevation in V1 and ST depression in V2 (highly specific for RV infarction)
- Isoelectric ST segment in V1 with marked ST depression in V2
- ST elevation in III > II
Diagnosis is confirmed by the presence of ST elevation in the right-sided leads (V3R-V6R)
- V1 is the only standard ECG lead that looks directly at the right ventricle
- Lead III is more rightward facing than lead II and hence more sensitive to the injury current produced by the right ventricle
Clinical Significance of RV Infarction
- RV infarction complicates up to 40% of inferior STEMIs (isolated RV infarction is extremely uncommon)
- These patients are very preload sensitive (due to poor RV contractility) and can develop severe hypotension in response to nitrates or other preload-reducing agents.
- Hypotension in right ventricular infarction is treated with fluid loading, and nitrates are contraindicated.
The ECG changes of RV infarction are subtle and easily missed!
Right-sided leads
There are several approaches to recording a right-sided ECG:
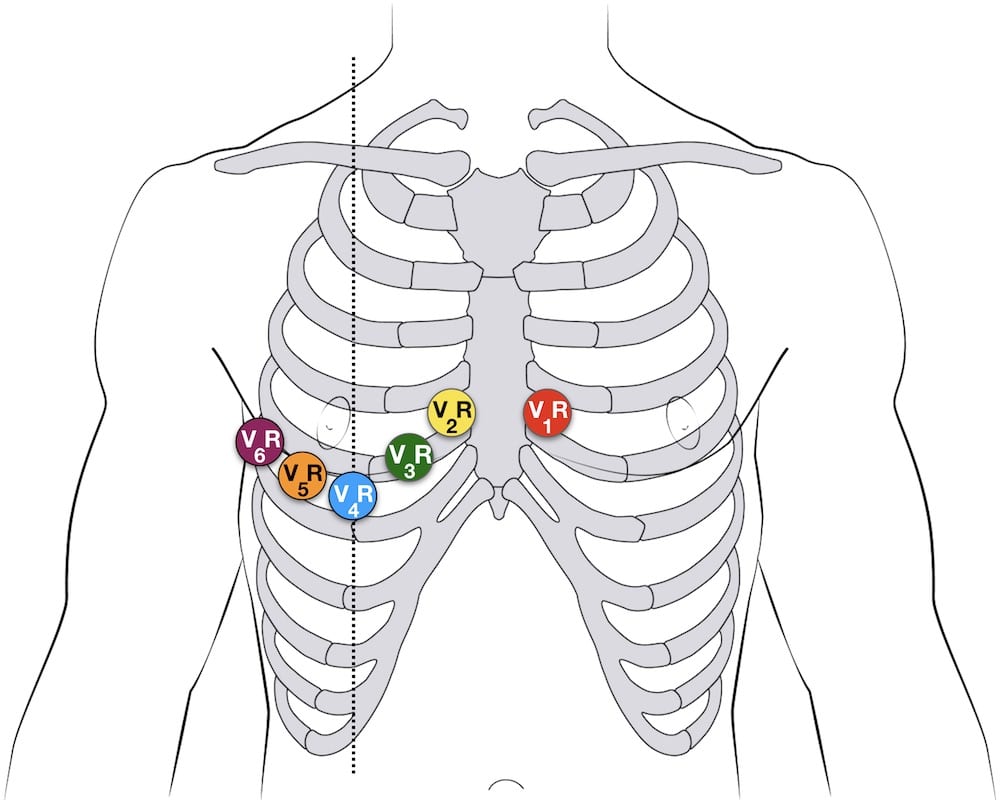
- A complete set of right-sided leads is obtained by placing leads V1-6 in a mirror-image position on the right side of the chest (see diagram below)
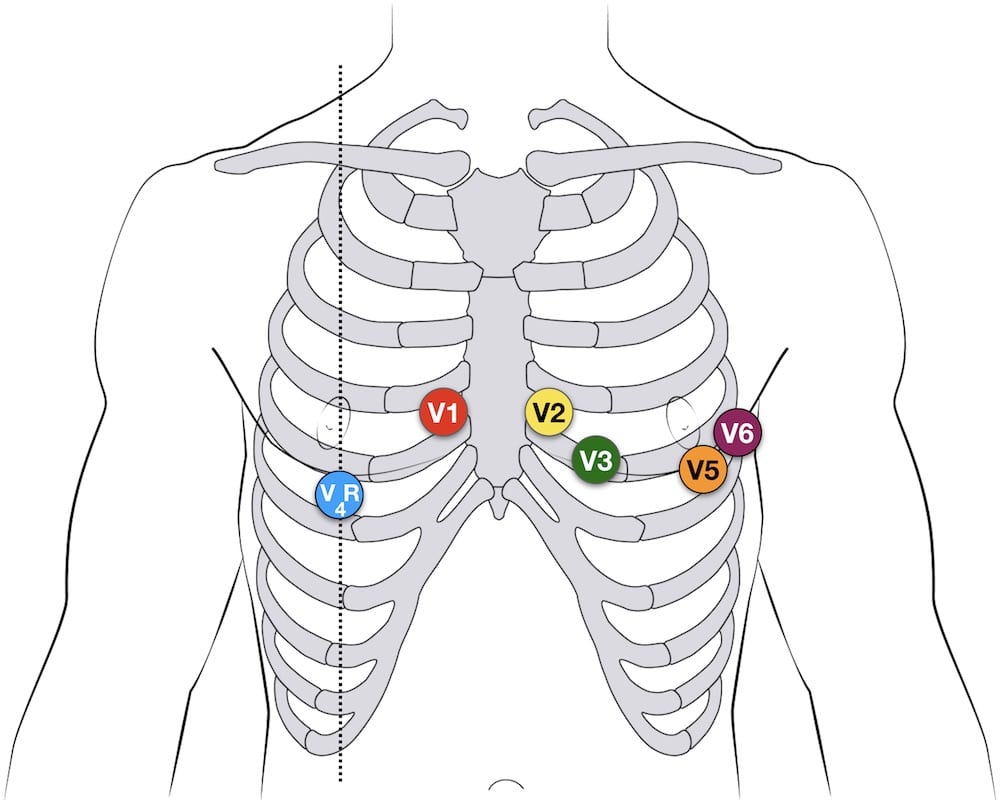
- It may be simpler to leave V1 and V2 in their usual positions and just transfer leads V3-6 to the right side of the chest (i.e. V3R to V6R)
- The most useful lead is V4R, which is obtained by placing the V4 electrode in the 5th right intercostal space in the mid-clavicular line
- ST elevation in V4R has a sensitivity of 88%, specificity of 78% and diagnostic accuracy of 83% in the diagnosis of RV MI
NB. ST elevation in the right-sided leads is a transient phenomenon, lasting less than 10 hours in 50% of patients with RV infarction.
Example ECG
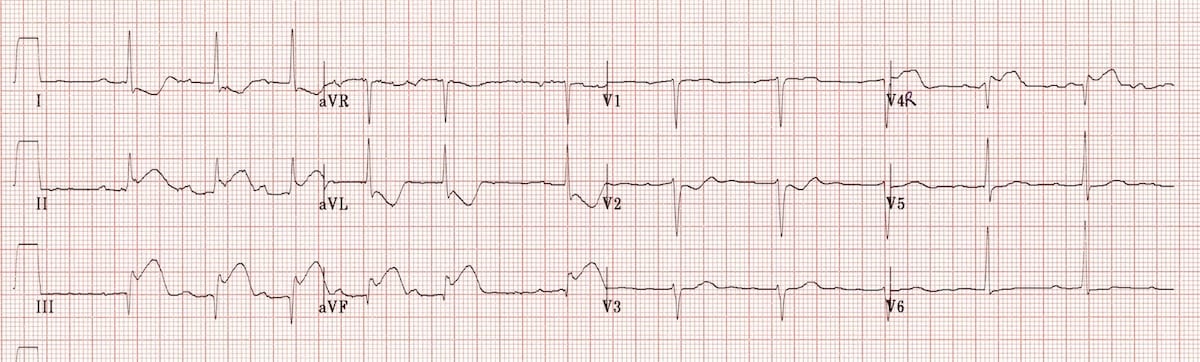
Example 1a
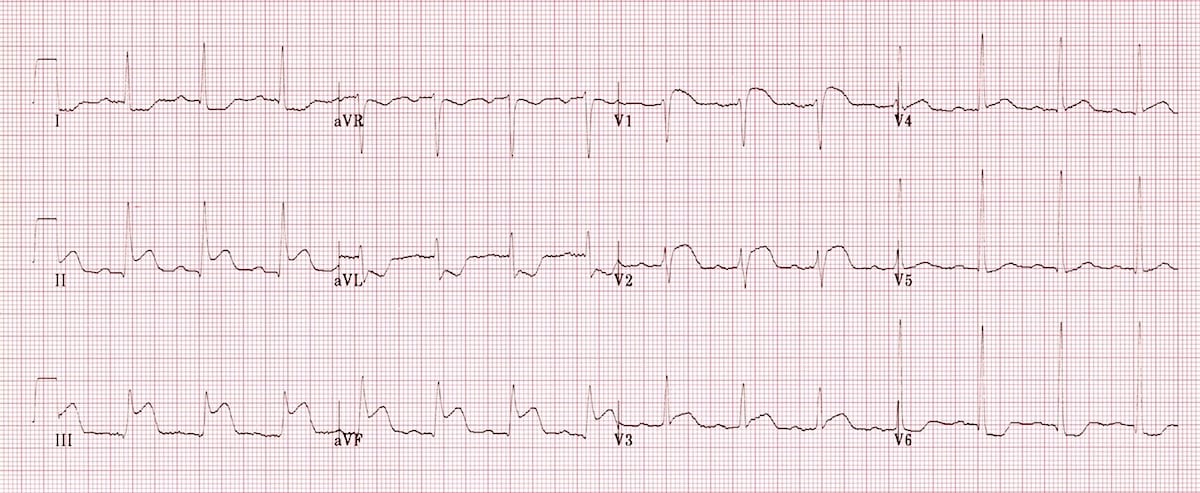
Inferior STEMI. Right ventricular infarction is suggested by:
- ST elevation in V1
- ST elevation in lead III > lead II
Example 1b
Repeat ECG of the same patient with V4R electrode position:
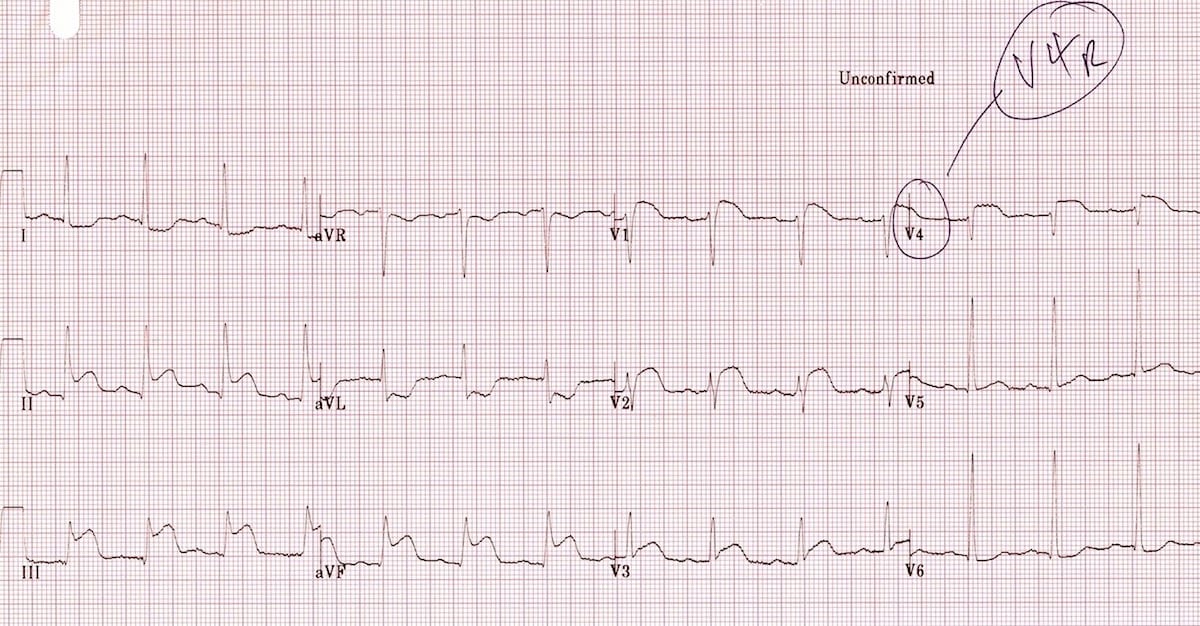
- There is ST elevation in V4R consistent with RV infarction
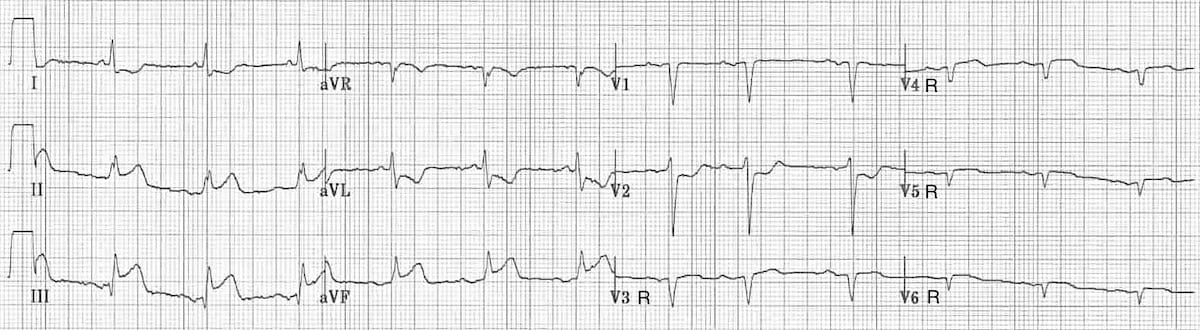
Example 2
Another example of right ventricular infarction in the context of inferior STEMI:
- ST elevation in lead III > lead II
- Isoelectric ST segment in V1 with marked ST depression in V2
- There is ST elevation in V4R.
Example 3
This ECG shows a full set of right-sided leads (V3R-V6R), with V1 and V2 in their original positions. RV infarction is diagnosed based on the following findings:
- There is an inferior STEMI with ST elevation in lead III > lead II
- V1 is isoelectric while V2 is significantly depressed
- There is ST elevation throughout the right-sided leads V3R-V6R
Example 4a
Try this one yourself…
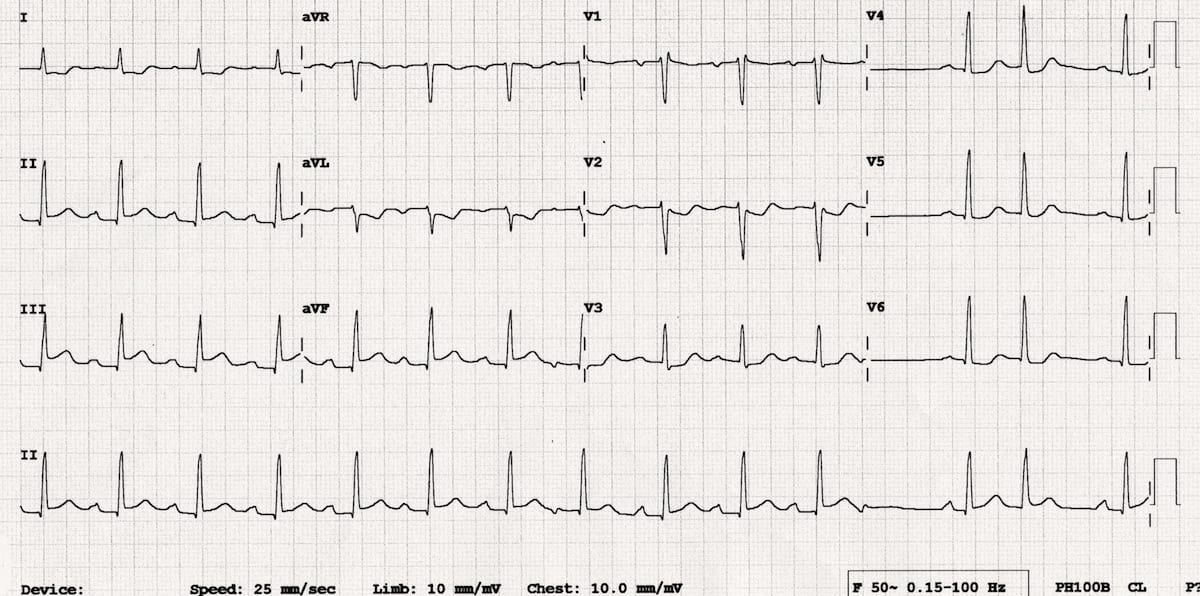
Reveal Interpretation
- Inferior STEMI with STE in III > II
- Reciprocal ST depression in aVL and I
- Isoelectric ST segment in V1 with ST depression in V2-3
- These findings are consistent with inferior STEMI due to RCA occlusion, plus likely associated RV infarction.
Example 4b
Same patient, 9 minutes later…
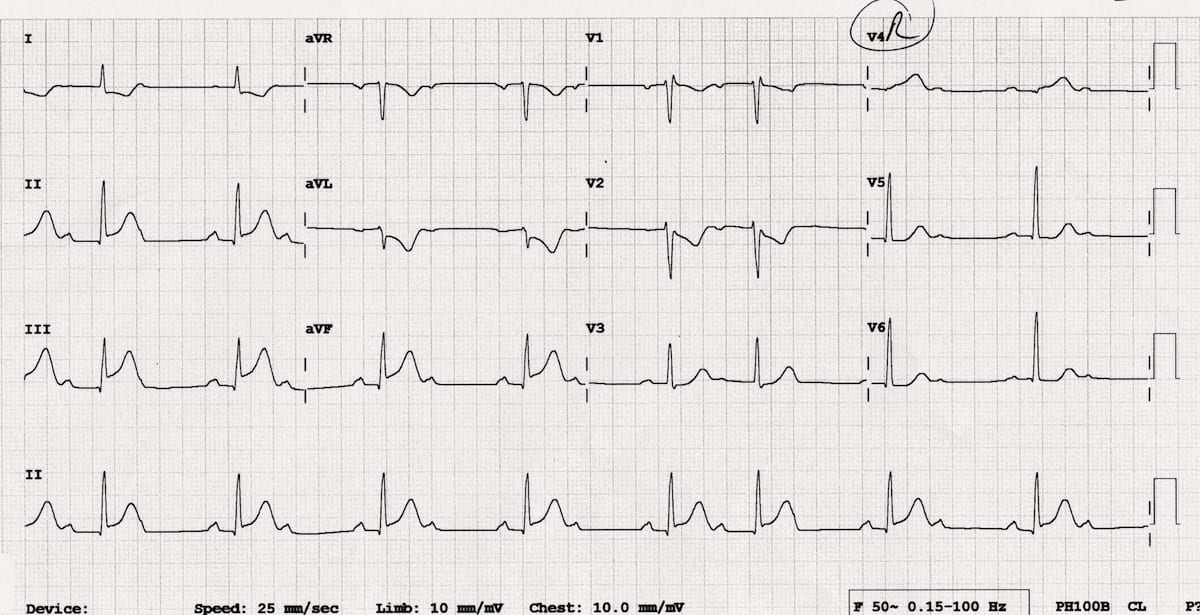
Reveal Interpretation
- Rapid evolution of inferior STEMI with dynamic increase in height of ST segments – this patient needs urgent PCI!
- V4R shows loss of R-wave height, significant ST elevation (> 0.5mm; ST segment > R wave) and hyperacute T wave (very large T wave given amplitude of QRS complex) – this confirms the diagnosis of RV MI
- Development of Wenckebach 2nd degree AV block indicates AV nodal ischaemia or a Bezold-Jarisch reflex (increased vagal tone often seen with inferior MI)
References
- Morris F, Brady WJ. ABC of clinical electrocardiography: Acute myocardial infarction-Part I. BMJ. 2002; 324: 831-4. [full text]
- Edhouse J, Brady WJ, Morris F. ABC of clinical electrocardiography: Acute myocardial infarction-Part II. BMJ. 2002; 324: 963-6. [full text]
Advanced Reading
Online
Textbooks
- Zimmerman FH. ECG Core Curriculum. 2023
- Mattu A, Berberian J, Brady WJ. Emergency ECGs: Case-Based Review and Interpretations, 2022
- Straus DG, Schocken DD. Marriott’s Practical Electrocardiography 13e, 2021
- Brady WJ, Lipinski MJ et al. Electrocardiogram in Clinical Medicine. 1e, 2020
- Mattu A, Tabas JA, Brady WJ. Electrocardiography in Emergency, Acute, and Critical Care. 2e, 2019
- Hampton J, Adlam D. The ECG Made Practical 7e, 2019
- Kühn P, Lang C, Wiesbauer F. ECG Mastery: The Simplest Way to Learn the ECG. 2015
- Grauer K. ECG Pocket Brain (Expanded) 6e, 2014
- Surawicz B, Knilans T. Chou’s Electrocardiography in Clinical Practice: Adult and Pediatric 6e, 2008
- Chan TC. ECG in Emergency Medicine and Acute Care 1e, 2004
LITFL Further Reading
Emergency Physician in Prehospital and Retrieval Medicine in Sydney, Australia. He has a passion for ECG interpretation and medical education | ECG Library |
MBBS DDU (Emergency) CCPU. Adult/Paediatric Emergency Medicine Advanced Trainee in Melbourne, Australia. Special interests in diagnostic and procedural ultrasound, medical education, and ECG interpretation. Co-creator of the LITFL ECG Library. Twitter: @rob_buttner