Sgarbossa: smaller amplitude leads have higher diagnostic yield
The diagnosis of occlusion myocardial infarction in intraventricular conduction delay (IVCD) can be challenging. We are often drawn to leads with large QRS complexes, such as V2-3 in this patient, to determine if the degree of ST-elevation seen is “acceptable”. However, it is often leads with small QRS complexes that will manifest subtle concordant or excessively discordant ST-segment changes.
LBBB v LAFB: improving definitions
The threshold of 120ms in defining LBBB was established in 1941 via animal model experimentation limited to limb leads, and not by objective measurements in humans. At this time, other causes of QRS prolongation such as LAFB or LVH were not yet appreciated. Despite this, the 120ms cut-off point has persisted to today, often leading to an overdiagnosis of bundle branch block. Some authors advocate redefining QRS duration in LBBB to > 130-140ms given the prolonged conduction deficits seen in comparison to other causes of IVCD.
The American Heart Association recommendations include “notched or slurred R wave in leads I, aVL, V5 and V6” as part of diagnostic criteria for LBBB, largely absent in this case. The ECG morphology seen in this patient is more consistent with LAFB due to prior anterior MI.
Diagnosing acute OMI in the setting of prior MI
Over half of patients will have persisting ST-elevation in precordial leads following anterior MI. This so-called LV aneurysm morphology is associated with a small T-wave amplitude:
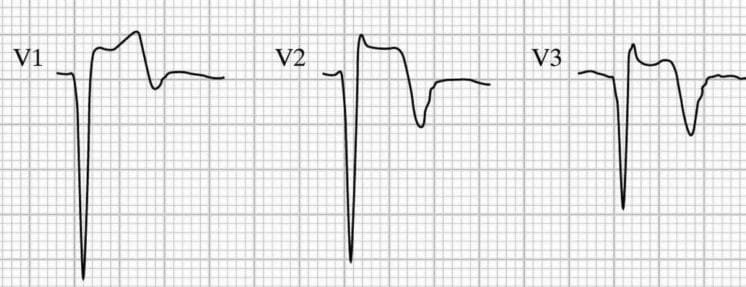
Differentiating LV aneurysm morphology from OMI can be difficult, and relies on clinical suspicion, reciprocal changes, and as discussed above, T wave amplitude relative to the QRS complex. Such reciprocal changes can be more difficult to ascertain in the context of IVCD. “Pseudonormalisation” of previously inverted T waves (such as V3 in the above example) can mask hyperacute T waves — previous ECGs are important in diagnosing OMI in these settings.
Summary
The subtlety of ECG findings in this patient, combined with his negative initial high sensitivity troponin and pain-free status on arrival, could have lead to a misdiagnosis of “unstable angina” and caused significant delays in potentially life-saving intervention.
- In IVCD, pay close attention to leads with small QRS complexes that will manifest subtle concordant or excessively discordant ST segment changes
- QRS duration > 120ms does not necessarily equal bundle branch block. Look for other features of LBBB to differentiate from LAFB and other causes of IVCD
- Hyperacute T-waves should always be interpreted in proportion to the preceding QRS amplitude
- A negative initial high-sensitivity troponin does not exclude ACS requiring emergent intervention