Right precordial T-wave inversion: Differentiating ACS and PE
With increasing awareness of the ECG changes of Wellens syndrome in recent years, it is easy for premature closure to occur in the diagnostic process with the above presentation. In patients with symptoms of ACS and right precordial T-wave inversion, we must always consider acute RV strain as a differential in addition to ischaemia/infarction.
The finding of associated T-wave inversion in leads III and V1 has demonstrated a high specificity (99%) for differentiating PE from ACS. When right precordial T-wave inversion is present, the clinician should be prompted to look for other ECG features suggestive of RV dilatation, including clockwise rotation and right axis deviation. In patients where clinical suspicion for PE is high, right precordial T-wave inversion may be a useful marker of severity, associated with massive PE and high pulmonary pressures.
![Evolution of T-wave inversion [A-D] after coronary reperfusion in STEMI reperfusion and in Wellens syndrome (NSTEMI)](https://litfl.com/wp-content/uploads/2018/08/Evolution-of-T-wave-inversion-A-D-after-coronary-reperfusion-in-STEMI-reperfusion-and-in-Wellens-syndrome-NSTEMI.png)
The type B pattern of Wellens syndrome typically presents with deep T-wave inversion. An episode of self-resolved chest pain and raised troponin implies infarction and reperfusion has occurred, and thus changes should be dynamic. Serial ECGs in this patient did not demonstrate change in T-wave morphology in right precordial leads, and the shallow nature of inversion seen is atypical for Wellens syndrome.
Understanding clockwise rotation
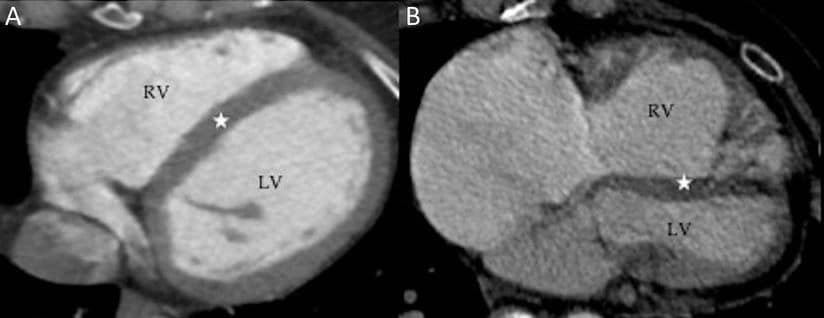
Right: RV dilatation and hypertrophy compressing the LV, creating “clockwise” rotation of the heart
The term “clockwise rotation” describes the apparent rotation of the heart as viewed from below in standard CT/MRI cross-sectional imaging views. High pulmonary pressures in PE cause acute RV pressure overload and dilatation, compressing the interventricular septum (IVS). Ensuing RV dysfunction and hypokinesis worsens these changes, particularly in the apical region. Leads V5-6, which usually face the LV wall and reflect LV depolarisation directly, are subsequently orientated over the IVS. The R/S transition point thus shifts rightwards towards V6.
What about SIQIIITIII?
The “classic” SIQIIITIII finding lacks supporting literature as a sensitive and/or specific marker for PE, but it’s individual components can serve as useful prompts to examine for other ECG features of PE.
A prominent S wave in lead I, as seen in this case, is simply a reflection of clockwise rotation and/or right axis deviation. T-wave inversion in lead III as an isolated finding can be a normal variant, but in the context of right precordial T-wave inversion is highly specific for PE. Similarly, Q waves in lead III may be a normal variant, or a reflection of regional RV ischaemia and/or infarction secondary to acute pressure overload.
Summary
- In patients with symptoms of ACS and right precordial T-wave inversion, associated T-wave inversion in leads facing the right ventricle (III and V1) is highly specific for PE
- Type B pattern of Wellens syndrome presents with deep, symmetrical T-wave inversion. In the context of chest pain and a raised troponin, ECG changes are usually dynamic
- ECG features of acute right heart strain simply reflect a sudden increase in pulmonary pressures, and can be seen in any cause of hypoxia due to pulmonary hypoxic vasoconstriction