Secundum ASD is a common sporadic congenital heart defect with a prevalence of around 1 in 800 in the general population. Patients with an isolated defect usually remain asymptomatic until the 3rd decade of life, with the most common adult presentation being supraventricular tachycardia (SVT), followed by exercise intolerance and/or fatigue. If left untreated, long term morbidity relates to the development of pulmonary hypertension.
ECG changes likely relate to functional RV volume overload due to left-to-right shunting, with resultant raised pulmonary pressures. The characteristic Crochetage sign often disappears following defect repair, which is usually via transcatheter device closure.
ECG features of secundum ASD
- Characteristic R wave notching in inferior leads (Crochetage sign)
- Slight right axis deviation (RAD)
- Voltage evidence of right ventricular hypertrophy (RVH), often in the form of “incomplete” right bundle branch block (RBBB)
Differentials for “SVT” in this patient
The term “SVT” is a misnomer commonly used synonymously with AVNRT, which is one of many forms of SVT. SVT refers to any tachyarrhythmia arising from above the level of the Bundle of His, and encompasses regular atrial, irregular atrial, and regular atrioventricular tachycardias.
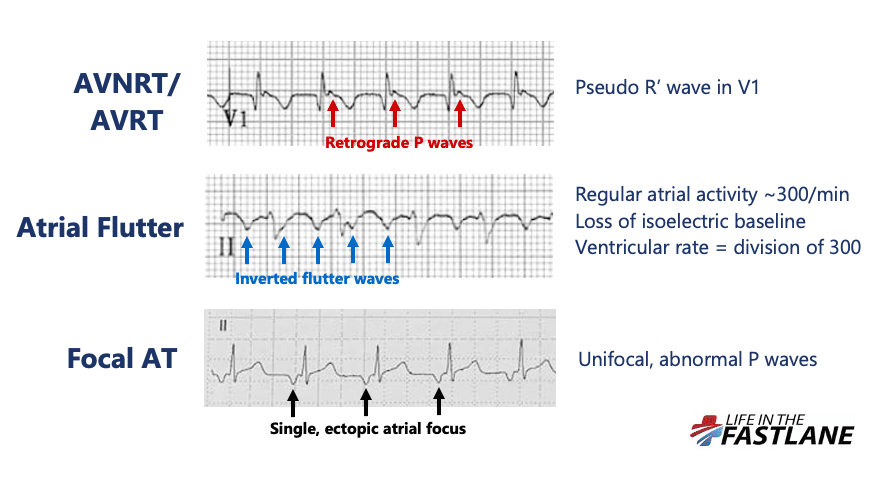
Differentials for a regular narrow complex tachycardia include:
The most common form of AVNRT (slow-fast) is precipitated by the arrival of a PAC whilst the AV node is still refractory. This leads to the formation of a re-entry circuit, which causes simultaneous anterograde activation of the Bundle of His and retrograde activation of the atria. Resultant HR will depend on the length of the re-entry circuit in the AV node which is variable between patients.
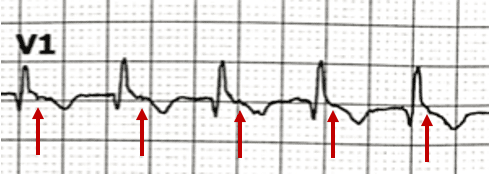
The presence of retrograde P waves on the ECG is variable – they may be buried within or after the QRS complex. The term pseudo R’ wave refers to the presence of a retrograde P wave visible in the terminal portion of the QRS complex, usually best seen in V1 or V2, which may mimic an RSR’ complex appearance. These can be very subtle.
Differentiation of AVNRT from atrial flutter on the ECG can be difficult and may not always be possible. Atrial flutter is caused by a similar re-entry circuit occurring within the right atrium. The length of this circuit corresponds to the size of the right atrium, usually resulting in flutter waves at a rate of ~300bpm. The ventricular rate depends on the AV conduction ratio. This ratio is often referred to as the “AV block”, however this is again a misnomer. Such AV bock is a physiological response to rapid atrial rates and implies a normally functioning AV node.
High grade AV conduction ratios in atrial flutter (4:1, 5:1), particularly with variable block, are often seen in the presence of AV nodal blocking drugs in the elderly population.
- When present in all three inferior leads, Crochetage sign is highly specific for the diagnosis of secundum ASD
- Commonly used to refer to AVNRT, SVT is a broad term encompassing regular atrial, irregular atrial, and regular atrioventricular tachycardias
- At rates of ~150bpm, differentiation of AVNRT versus atrial flutter can be difficult. Look for pseudo R’ waves in V1 suggestive of AVNRT, or consider the use of adenosine which will revert AVNRT or unmask flutter waves in atrial flutter