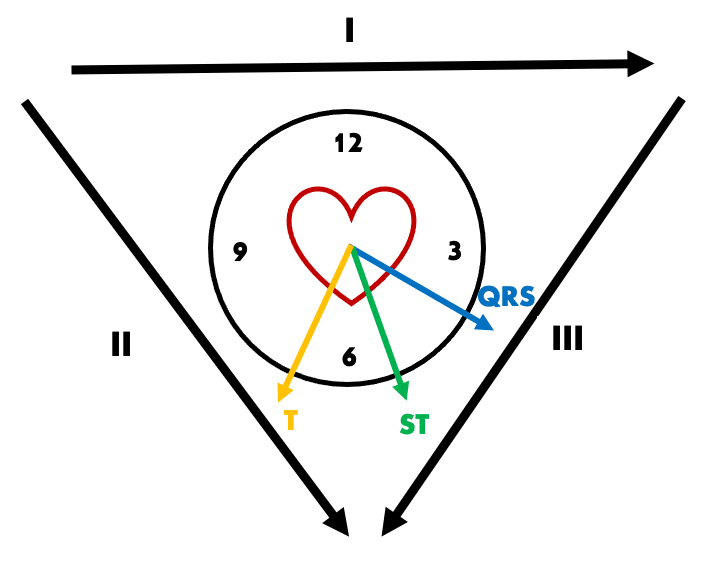
QRS-T wave angle as a marker of ischaemia
aVL is the only lead truly reciprocal to the inferior wall, and we often examine this lead closely for ST-T changes in suspected inferior OMI. Although ST depression in aVL is common in inferior OMI, it may not be evident at early stages of infarction. In our patient above, pathological T wave inversion in aVL precedes any other reciprocal change. We know that T-wave inversion in aVL can be a normal variant, and last week we discussed the QRS-T wave angle as an additional tool for differentiating such benign versus ischaemic T wave inversion.
In our patient above, QRS axis is + 30 degrees and T wave axis + 120 degrees, giving a QRS-T wave angle of 90 degrees. Such a wide angle (> 45 degrees) suggests T-wave inversion seen in lead I and aVL is pathological and due to a primary repolarisation abnormality of inferior infarction.
AV block in inferior MI
Varying degrees of AV nodal block are common in inferior MI, as the AV node is supplied by the RCA in approximately 80% of the population. 20% of patients with inferior OMI will develop 2nd or 3rd degree AV block — around half of these will demonstrate a step wise progression as with our patient above, with the other half suffering abrupt onset.
Such blockade may be subtle in early stages, especially as these patients do not always manifest bradycardia due to concurrent sympathetic drive from pain and ischaemia. Identifying such AV blockade may assist in making the early diagnosis of inferior OMI, and allow us to monitor for progression to fatal bradyarrhythmias.
Note: SA nodal dysfunction is also common in inferior OMI, as the SA node is supplied by the RCA in the majority (60%) of patients. Manifestations include sinus bradycardia, sinus pauses, or SA block.
“Flattened” V2 and RV infarction
Most “normal” ECGs demonstrate some degree of ST elevation in right precordial leads, especially V2-3. A completely isoelectric ST segment as seen in our patient’s first ECG is abnormal and indicates a relative degree of ST depression.
In the absence of dedicated right-sided leads, V1 is the only standard ECG lead that looks directly at the right ventricle. Any degree of ST depression in V2 relative to V1 is suggestive of right ventricular infarction (note that V1 will not always manifest ST elevation).
- In the early stages of inferior OMI, ST segment changes will not always be evident. Examine for other suggestive ECG features including reciprocal change in aVL, AV blockade, and flattening of the ST segment in V2 relative to V1
- Reciprocal ST depression in aVL may be preceded by T-wave inversion. The QRS-T wave angle can assist us to determine if such T-wave inversion is normal variant or due to evolving inferior infarction
- If in doubt, obtain serial ECGs early, ideally every 10 minutes in the initial assessment period!